
How Does Manual Therapy Work?
It’s not just clicks and pops


Photo by Toa Heftiba on Unsplash
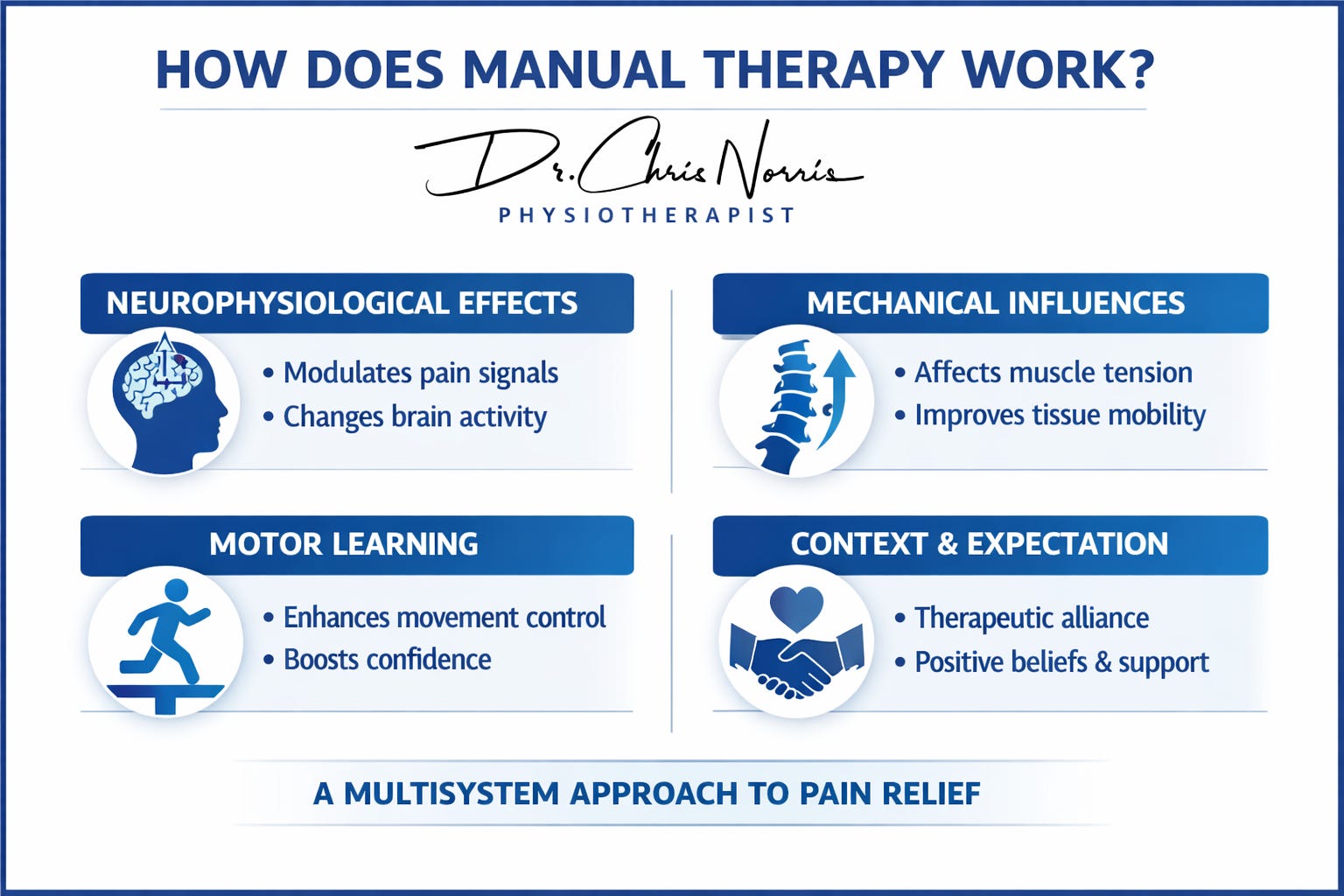
Manual therapy (MT) has long been central to musculoskeletal care, yet its mechanisms are now understood in far broader terms than the old “clicks and pops” explanation. Traditional models emphasised structural correction—realigning joints or breaking adhesions, for example—but modern research shows MT acts through a multisystem approach, combining neurophysiological, mechanical, and motor‑learning processes. This effect is further shaped by context, communication, and patient expectations. So, it’s not just local effects on the body region being treated; MT is affecting the whole person.
1. Manual Therapy Is Not Primarily Mechanical
“MT influences physiology, not structure.”
With hands-on therapy techniques, forces applied at the skin surface do not reposition joints or tissues in any meaningful way. The “pop” sometimes heard during manipulation occurs at several spinal levels, not just the targeted segment, and any stiffness reduction is short‑term and neuromuscular (related to how muscles are controlled by nerves) rather than structural. The hands-on technique is having an effect, but it’s not restricted to the part of the patient’s body being touched.
A 2025 living systematic review found low evidence for biomechanical tissue change but moderate evidence for neurovascular (blood flow) and neurological (nerve-related) effects, so the evidence is there (1).
2. Neurophysiological Mechanisms: The Core of Modern MT
MT provides controlled sensory input (touch) that modulates nociception (feeling pain) at both spinal and cortical levels. Within the spine (segmentally), it reduces dorsal‑horn sensitisation, alters motoneuron excitability, and affects sympathetic activity (1, 3).
Within the brain, imaging shows changes in cortical excitability, sensorimotor integration, and connectivity within pain‑processing networks; in other words, the brain is calmed down and works better. These effects underpin descending inhibition and neuroplasticity, especially in patients with mechanical pain or central sensitisation (1, 4).
In short, MT changes how the nervous system interprets and responds to sensory information.
3. Autonomic and Visceral Responses
MT can even temporarily influence blood pressure, breathing patterns, and lymphatic flow. These short‑term systemic effects support the concept of MT as a whole‑body stimulus, not a local mechanical fix (3).
4. Motor Control and Learning Effects
Another effect hinges on psychology. Drawing on the OPTIMAL theory of motor learning (which emphasises autonomy, positive expectations, and an external focus of attention), MT can be given in a way which gives the patient a sense of choice and involvement in their treatment. When done in this way, it helps reduce protective muscle guarding, improve movement confidence, and enhance sensorimotor integration. This creates a brief window where movement feels easier and safer, allowing exercise to be more effective (1).
“Think of MT as input; exercise as output.”
5. Context, Communication, and Expectation
MT is a shared encounter between a patient and practitioner, not merely a technique. Touch, beliefs, and the relationship (alliance) between therapist and patient can all actively shape outcomes. Expectation and context can amplify or diminish MT’s physiological effects (1).
The clinical environment—lighting, privacy, cultural sensitivity—also contributes to perceived safety and comfort, helping or hindering the MT effect.
6. What Manual Therapy Actually Does
So, in summary, MT delivers controlled sensory input that modulates pain, muscle tone, autonomic function, and motor control through neurophysiological mechanisms. It does not realign joints or break adhesions!
Key effects include:
Modulating pain signals (1) and influencing brain activity (4)
Affecting autonomic responses (3)
Improving movement confidence and control (1)
Enhancing therapeutic alliance and self-efficacy (1)
Reducing maladaptive beliefs and fear avoidance (1)
Promoting short-term tone reduction and relaxation to support rehabilitation (1)
7. Clinical Implications for Therapists
MT works best when combined with education, exercise, behavioural strategies, and self-management. Rather than a standalone fix, it is better viewed as a catalyst for change.
Therapists should try to identify likely responders—patients with mechanically provoked pain, those with a hyper-responsive nervous system (central sensitisation), or patients moving awkwardly (movement dysfunction)—and prioritise safety, comfort, and efficiency of techniques (1).
Use MT strategically: minimal effective dose, maximum patient involvement, and real-time feedback.
8. What This Means for Patients
MT is not about “cracking things back into place.” It helps the nervous system feel safer and the body to move better. The effects are real, measurable, and supported by modern science—especially when MT is combined with active rehabilitation.
9. The Shift in Perspective
This evolution from Traditional MT (patho‑anatomical, clinician‑centred) to Contemporary MT (person‑centred, biopsychosocial) reflects a broader professional identity within the therapy world: empathy, communication, and outcome‑focused reasoning.
MT remains hands‑on, but its power lies in how those hands communicate safety and possibility.
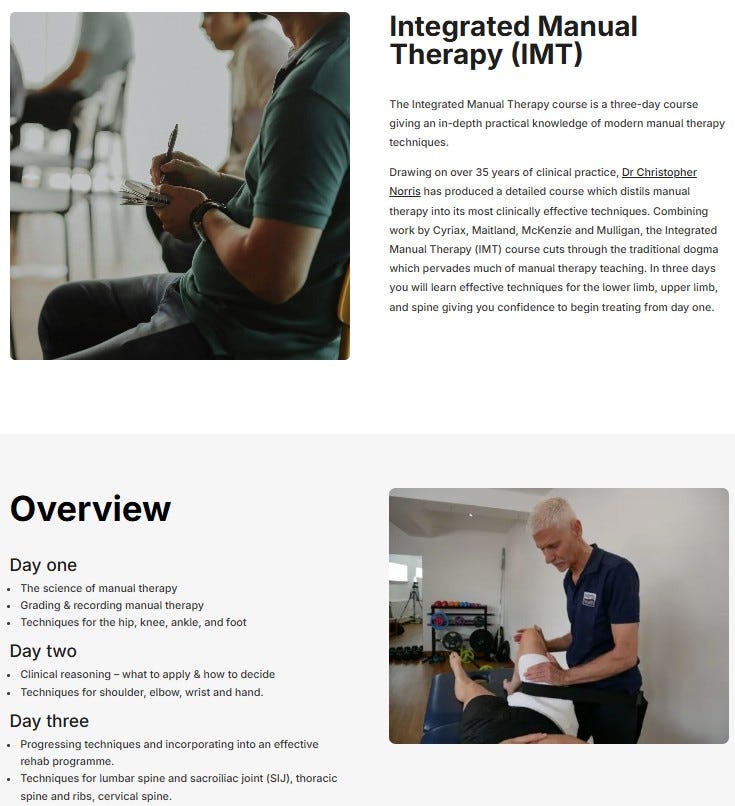
Continuing Professional Development
Interested in developing these skills further?
Explore Dr Chris Norris’ 3‑day CPD course, “Integrated Manual Therapy” — an evidence‑based, highly practical programme linking neurophysiology, movement retraining, and clinical reasoning. CLICK HERE
References
1. Keter, D. L., Bialosky, J. E., Brochetti, K., et al (2025). The mechanisms of manual therapy: A living review of systematic, narrative, and scoping reviews. PLoS One, 20(3), e0319586.
2. Evans, D. W., & Breen, A. C. (2006). A biomechanical model for spinal manipulation. Journal of Manipulative and Physiological Therapeutics.
3. Alanazi, M. S., Degenhardt, B., Kelley‑Franklin, G., et al. (2024). Autonomic nervous system and viscera‑related responses to manual therapy: A narrative overview. International Journal of Osteopathic Medicine, 54, 100735.
4. Manual therapy and neuroplasticity: Central mechanisms and clinical implications for pain relief. (2025). Journal of Manual & Manipulative Therapy, 33(4), 283–285.
5. Norris, C. M. (2019). Sports and Soft Tissue Injuries (5th ed.). Routledge.